INVESTIGATED BY SCIENTISTS – ENCEPHALITIS AND FATALITY AFTER STANDARD VACCINE
Illness after the Measles, Mumps, and Rubella vaccine
We bring to your attention a published research article about a healthy 13-month-old boy who received the standard vaccine for Measles, Mumps, and Rubella (MMR), then became severely ill and died.
We’ll tell you how it happened, how it was investigated, what the researchers learned, and most importantly, how you can make better-informed health decisions for the safety of your loved ones.

How it Happened
This 13-month-old boy had received all other recommended childhood vaccines, including the Tuberculosis vaccine (also known as the BCG vaccine), all with no apparent side effects. But after receiving the first dose of the Measles, Mumps, and Rubella vaccine, he developed a skin rash at the injection site. Often called ‘mini-measles’, this type of reaction is reported to be a “relatively infrequent but established complication” of the Measles, Mumps, and Rubella vaccine, that usually goes away on its own. (1)
However, with the skin rash continuing on the 6th day after the vaccine, the infant was brought to the hospital. In the next 5 days, he recovered enough to be discharged. But after discharge, during the next four days, the rash came back and he developed a fever. So he was brought back to the hospital and re-admitted.
Tests revealed issues related to his heart, blood, and sodium levels. They also diagnosed Hepatitis, which is a serious inflammation of the liver. The child then started to have seizures. Doctors were not able to control the seizures with medication. So on the fifth day of his hospital stay, the boy was transferred to the pediatric intensive care unit (PICU), where he was sedated and placed on a ventilator.
Doctors tested his blood for other disorders, including allergies and autoimmune diseases. (See ‘Table S3’ below, from the original published research article.) The results of this standard ‘immunological’ testing were all normal.
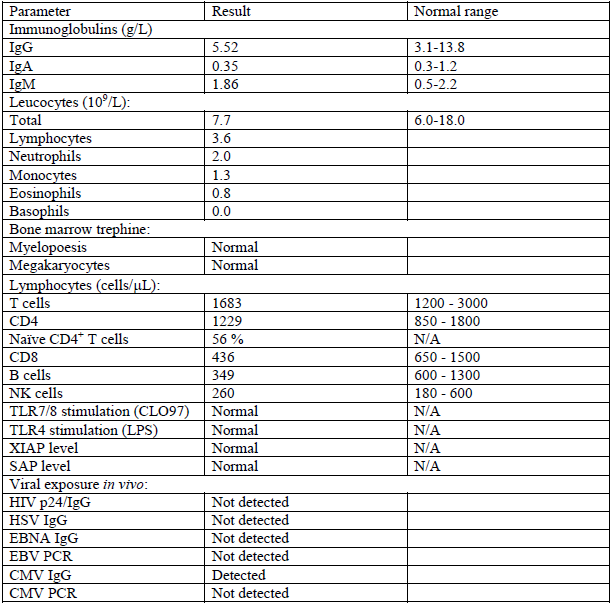
NK = natural killer, TLR = Toll-like receptor, LPS = lipopolysaccharide, XIAP = X-linked inhibitor of apoptosis protein, SAP = SLAM-associated protein, HIV = human immunodeficiency virus, HSV = herpes simplex virus, EBNA = Epstein-Barr virus (EBV) nuclear antigen, PCR = polymerase chain reaction, CMV = cytomegalovirus. Tests were performed at various time points after presentation: immunoglobulins, day 22, baseline full blood count, day 20; lymphocyte subsets, day 22, TLR stimulation, day 50, XIAP/SAP, day 50, viral serology, day 21. (1)
Hospital Treatments and Tests
To combat suspected diseases, doctors then treated the infant with intravenous (IV) drugs, including:
- Antibiotics – possibly for bacterial infections
- Antivirals – possibly for viral infections
- Immunoglobulins – possibly to reinforce the immune system
- High-dose corticosteroids – possibly to lower inflammation
More tests included Magnetic Resonance Imaging – or MRI – of the brain. The results were abnormal, revealing inflammation on both sides of his brain.
The child’s spinal fluid was tested, revealing active Herpes virus and Measles virus.
The Mumps virus was found in the boy’s urine, indicating that the vaccine virus was now widespread in his body. In fact, an active Rubella virus was also detected, which had been introduced by a previous vaccine.
At one point, the child was taken off the ventilator, but seizures resumed. He was diagnosed with severe neurological injury, and his overall condition continued to deteriorate.
According to the research article, on Day 81 – less than 3 months after the Measles, Mumps, and Rubella vaccine was injected – “the patient succumbed to this catastrophic illness.” (1)
The research article states that this little boy “developed severe, prolonged and ultimately fatal encephalitis, as a complication of MMR vaccination.” (2)

Why Did This Happen?
Prior to the vaccine, the child had not shown any signs of abnormal response to the virus.
After his death, many crucial questions remained to be investigated.
Why did all this happen in this little boy’s seemingly healthy body – after a routine childhood vaccination?
Importantly, answers might help the family understand, and could possibly help other children.
Answers might also advance our understanding of possible complications of virus vaccines.
Before we delve into these answers, it’s important to review some basics about the vaccine this child received.
What Vaccines Do?
Vaccines are supposed to teach your body’s immune system how to fight off certain invading germs, in order to avoid the serious illnesses that those germs cause. Scientists make vaccines in several different ways, so there are several different types of vaccines. (3)
Live-attenuated Vaccines
This 13-month-old child was injected with a vaccine of the ‘live attenuated’ type. Live vaccines are made with attenuated – or weakened forms – of the germs that cause the diseases.
The vaccine that this infant received actually contained live Measles, Mumps, and Rubella viruses. The ‘live virus’ MMR vaccine is routinely given to children in the U.S. and in many other countries.
How Should these Live Virus Vaccines Work?
Live virus vaccines are very similar to the natural virus infection. They are supposed to trigger the immune system to create a strong and long-lasting response that will fight the target viruses. One or two doses of live virus vaccines are supposed to give a lifetime of protection. (3)
What are Some Risks?
Live vaccines are also widely given to protect against:
- Rotavirus – See “Who should not get the Rotavirus vaccine?”
- Smallpox – See “You are more likely to have serious side effects if:”
- Chickenpox – See “Who should not get the chickenpox vaccine?”
- Yellow fever – See “Who should not get the yellow fever vaccine?”
Warnings on the website of the U.S. Department of Health & Human Services (HHS) alert us to some “limitations” of these live attenuated virus vaccines. For example:

“Because they contain a small amount of the weakened live virus, some people should talk to their health care provider before receiving them, such as people with weakened immune systems, long-term health problems, or people who’ve had an organ transplant.” (3)
Additionally, HHS warns us about the risks related to the distribution and quality of live virus vaccines:

“They need to be kept cool, so they don’t travel well. That means they can’t be used in countries with limited access to refrigerators.” (3)
But this child was treated in a contemporary medical facility in the UK, so the quality of the vaccine was likely not an issue.
The Investigation
The Lead Research Physician assembled a team of highly specialized doctors, scientists, and clinical researchers. With their deep understanding of biology, genetics, immunology, and diagnostics, they focused on studying the child’s genes. They followed strict scientific methods. They applied cutting-edge testing techniques. And they thoroughly documented all aspects of their investigation.
The team followed best-practice scientific standards. According to the research article, “…analyses were performed in accredited regional diagnostic laboratories to standard protocols.” (2)
Why was This Vaccine Virus Lethal?
Doctors had detected both Mumps and Rubella viruses in the child’s brain more than 7 weeks after the MMR vaccination. [This is clearly not a normal response to the vaccine.]
Researchers used a genetic testing technique called ‘targeted resequencing’. And they identified a crucial genetic mutation. That specific mutation affects the entire body’s ability to defend against viruses. So when the live virus vaccine was injected into this child’s body, the genetic mutation compromised that virus defense.
In Scientific Terms, Here’s a Quick Summary:
This child’s genetic mutation caused a deficiency of the ‘interferon-α/β receptor’ also known as IFNAR2.

The IFNAR2 receptor normally plays a critical role in our bodies’ fight against viruses and other threatening invaders.
It is part of the human ‘interferon pathway’ that normally keeps viruses under control.
So what went wrong?
Through further testing and confirmation, the researchers determined that this mutation – the genetic deficiency of IFNAR2 – was the underlying cause of the infant’s severe encephalitis and ultimate death. Because of this deficiency, the child was not able to adequately fight the ‘live attenuated’ viruses that were introduced by the MMR vaccine. Unable to fight the vaccine viruses, they grew and overpowered his system. He eventually succumbed to all the virus-induced illnesses.
Summary Research Remarks
The research article summary warns readers that this genetic deficiency in the Interferon pathway is possibly fatal.
They go on to state that Interferon α/β is “vital” to viral immunity – fighting certain illnesses.
“Human IFNAR2 deficiency causes fatal susceptibility to live viral vaccines, revealing a vital but narrow nonredundant role for IFN-α/β in viral immunity.” (4)
Curious About Interferons
We find it interesting that when the Authors wrote this research article, they used the word ‘narrow’ to describe the role of Interferon α/β.
Choosing the word “narrow” makes us quite curious to learn more about how Interferons work in the body – and what happens when doctors use them outside of this “narrow” role when treating illnesses such as Hepatitis B and C, Cancers, and Multiple Sclerosis. Interferons are even being used to treat other viruses, including Corona.
Interferon-induced illnesses such as Thyroid disorders, Autoimmune diseases, and Psychiatric issues have been reported for decades in the medical literature. Separately, we will continue to dive deeper into the important topic of Interferons and their profound effect on many aspects of our health.
Learn More About Vaccines
We encourage you to explore FDA.gov to learn more about the Vaccines Licensed for Use in the United States.
Review the Facts
We invite you to explore and verify the facts in the Authors’ original research article – full text (PDF download).
Below you will find article excerpts and links to the published article, along with the formal citation and list of Authors with their professional Affiliations.
Please review this information so that you can make more informed decisions for the health and safety of your family and loved ones.
Gratitude to the Family, Scientists, Clinicians and Researchers
We appreciate the patient’s family, and each of the Authors and members of the research team for their groundbreaking scientific work, and for making this important clinical information publicly available.
Understanding of this work greatly benefits not only the scientific community, but also individuals, parents and families all over the world.
The following excerpts were taken from the research article published by scientists, clinicians and researchers at UK’s Newcastle University Medical School, led by Dr. Christopher J. A. Duncan and a team of clinical researchers in their 2015 article entitled;
“Human IFNAR2 deficiency: Lessons for antiviral immunity”
Type I interferons in antiviral defense
“…We report the case of a child and a newborn sibling with a homozygous mutation in the high-affinity interferon-α/β receptor (IFNAR2), which prevented cells from responding to IFN-α/β. The previously healthy proband developed fatal encephalitis after exposure to the live attenuated measles, mumps, and rubella vaccine. Reconstituting the proband’s cells with IFNAR2 restored control of IFN-attenuated viruses…” (4)
Abstract
“…We investigated a previously healthy child with fatal encephalitis after inoculation of the live attenuated measles, mumps, and rubella (MMR) vaccine. By targeted resequencing, we identified a homozygous mutation in the high-affinity IFN-α/β receptor (IFNAR2) in the proband, as well as a newborn sibling, that rendered cells unresponsive to IFN-α/β. Reconstitution of the proband’s cells with wild-type IFNAR2 restored IFN-α/β responsiveness and control of IFN-attenuated viruses. Despite the severe outcome of systemic live vaccine challenge, the proband had previously shown no evidence of heightened susceptibility to respiratory viral pathogens…” (4)
Summary:
“Human IFNAR2 deficiency causes fatal susceptibility to live viral vaccines, revealing a vital but narrow nonredundant role for IFN-α/β in viral immunity.” (4)
CITATION:
Duncan, Christopher & Mohamad, Siti & Young, Dan & Skelton, Andrew & Leahy, Timothy & Munday, Diane & Butler, Kiana & Morfopoulou, Sofia & Brown, Julianne & Hubank, Mike & Connell, Jeff & Gavin, Patrick & McMahon, Cathy & Dempsey, Eugene & Lynch, Niamh & Jacques, Thomas & Valappil, Manoj & Cant, Andrew & Breuer, Judith & Hambleton, Sophie. (2015). Human IFNAR2 deficiency: Lessons for antiviral immunity. Science Translational Medicine. 7. 307ra154-307ra154. 10.1126/scitranslmed.aac4227.
Sources:
- Supplementary Materials PDF download: https://www.science.org/doi/suppl/10.1126/scitranslmed.aac4227/suppl_file/7-307ra154_sm.pdf U.S. Department of Health &
- Full published report PDF download:
https://research-repository.st-andrews.ac.uk/bitstream/handle/10023/7692/aac4227_ArticleContent_revised_clean.pdf - Human Services (HHS):
https://www.hhs.gov/immunization/basics/types/index.html - Abstract and References:
https://www.science.org/doi/10.1126/scitranslmed.aac4227
https://pubmed.ncbi.nlm.nih.gov/26424569/
Authors and Affiliations:
C.J.A. Duncan1,2*, S.M.B Mohamad1,3, D.F. Young4, A.J. Skelton5, T.R. Leahy6, D.C. Munday4, K.M. Butler6, S. Morfopoulou7, J.R. Brown8,9, M. Hubank10, J. Connell11, P.J. Gavin6, C. McMahon12, E. Dempsey13, N.E. Lynch14, T.S. Jacques15, M. Valappil16, A.J. Cant1,17, J. Breuer7,8, K.R. Engelhardt1, R.E. Randall4, S. Hambleton1,17*.
1 Primary Immunodeficiency Group, Institute of Cellular Medicine, Newcastle University, Newcastle upon Tyne, NE1 4LP, United Kingdom
2 Department of Infectious Diseases and Tropical Medicine, Royal Victoria Infirmary, Newcastle upon Tyne, NE1 4LP, United Kingdom
3 Advanced Medical and Dental Institute, Universiti Sains Malaysia, 11800 Penang, Malaysia
4 School of Biology, University of St. Andrews, St. Andrews, Fife, KY16 9ST, United Kingdom
5 Bioinformatics Support Unit, Newcastle University, Newcastle upon Tyne, NE1 4LP, United Kingdom
6 Department of Pediatric Infectious Diseases and Immunology, Our Lady’s Children’s Hospital, Crumlin, Dublin 12, Ireland
7 Division of Infection and Immunity, University College London, London WC1E 6BT, United Kingdom
8 Virology Department, Great Ormond Street Hospital for Children NHS Foundation Trust, London WC1N 3JH, United Kingdom
9 NIHR Biomedical Research Centre, Great Ormond Street Hospital for Children NHS Foundation Trust, London WC1N 3JH, United Kingdom
10 Molecular Haematology and Cancer Biology Unit, Institute of Child Health, University College London, London WC1E 6BT, United Kingdom
11 National Virus Reference Laboratory, University College Dublin, Belfield, Dublin 4, Ireland.
12 Department of Pediatric Intensive Care and Anaesthetics, Our Lady’s Children’s Hospital, Crumlin, Dublin 12, Ireland
13 Department of Neonatology, Cork University Maternity Hospital, Wilton, Cork, Ireland
14 Department of Pediatrics, Bon Secours Hospital, Cork, Ireland
15 Department of Histopathology, Great Ormond Street Hospital for Children NHS Foundation Trust, London WC1N 3JH, United Kingdom
16 Public Health England, Royal Victoria Infirmary, Newcastle upon Tyne NE1 4LP, United Kingdom
17 Pediatric Immunology Service, Great North Children’s Hospital, Newcastle upon Tyne NE1 4LP, United Kingdom
*Correspondence to: [email protected] or [email protected]